
Auto Accidents
Whiplash injury occurs when the body reacts to a deceleration or acceleration force by hyperflexion or hyperextension of the neck.
Whiplash injuries are very common in car accidents. The whiplash injury is in part due to the fact that the muscles do not have enough time to brace. Whiplash, or “Cervical Acceleration/Deceleration” (CAD) accidents most often occur when a patient is stopped at a light or a stop sign and is rear-ended. Often is the case where a car skids and slams into another car or pole and still another common scenario is when a person is driving and gets “T-Boned” by another moving vehicle in the side. *MVC=motor vehicle crash.
Uncomplicated cases of whiplash are the result of sprained ligaments in the neck. The muscles naturally spasm as a protective mechanism. Pain from the whiplash may be a stiff neck and may go down one or both arms. The sudden jerking motion of the head either front to back or side-side forces muscles and ligaments supporting the spine and head to move past their normal physiological limit and can thus be overstretched or torn. Additionally, vertebrae can be forced out of their normal alignment thus reducing range of motion (ROM).
Interestingly, in some extreme cases, the neck muscles and ligaments are so damaged and stretched that a patient’s ROM actually exceeds all normal ranges. Additionally, the actual spinal cord and/or nerve roots in the neck can get stretched and irritated causing even more pain that we call “radiculopathy.” All of this damage and instability can result in pain in the entire neck (cervical spine), mid-back (thoracic spine) and even the low back (lumbar spine). Patients will often complain of headaches, dizziness, blurred vision, face pain, nausea, shoulder pain, knee pain and a other seemingly unrelated health issues. Be advised that all these symptoms are normal after a MVC (motor vehicle crash).
*NB: Most of the citations on this page have been duplicated with actual experiments or cited in Foreman & Croft, Whiplash Injuries: Cervical Acceleration/Deceleration Syndrome, 3rd Ed., Lippincott Williams & Wilkins, 2002. **cervical acceleration/deceleration can be shortened to CAD.

Whiplash Statistics:
The numbers are shocking. Each year in the U.S., about 3 MILLION people experience whiplash neck and back injury. This should indicate to anyone, the sizable nature of this issue and what a public health problem whiplash has become. Actually, a further analysis of the 3 Million people shows that number is about HALF of all who are actually exposed to these types of trauma. Of the 3 Million, about 1.5 million will eventually recover. Another 600,000 will continue to have long-term symptoms and pain and another 150,000 will become disabled to one degree or another, each year as a direct result of Whiplash. Research has shown that nearly half (45%) of all Americans with chronic neck pain attribute the pain to car accidents with Whiplash being the most commonly cited problem. (Ibid.)
According to both the US Dept. of Transportation (USDOT) and the
National Highway Traffic Safety Administration (NHTSA), traffic
accidents can be broken down this way---
On average, from year to year, Motor Vehicle Crashes (MVCs) in the U.S.
are statistically similar:
- 6,000,000 total accidents per year
- 3,000,000 claimed injuries per year
- 42,500 deaths per year
- 2,000,000 of the claimed injuries result in permanent damage to some part of the body
- Every 12 minutes, a person dies in a MVC
- Every 14 seconds, someone is injured in a MVC
- Accidents are largely the result of
- Drunken drivers (40%)
- Speeding (30%)
- Reckless driving (33%)
Examination:
Chiropractors are leaders among the professions in treating uncomplicated CAD injuries. A thorough case history is taken along with a thorough examination. Often is the case where X-Rays are indicated. According to the literature (Foreman,S., Croft, A., Ibid; and Yochum, T, Rowe, L, “Essentials of Skeletal Radiology”, 3rd Ed., Vol. 1, Lippincott Williams & Wilkens, 2005), with cervical trauma the “rule of seven” is observed. That is to say, the seven view Davis Series, is the norm and usually required to appreciate all aspects of the cervical spine after ballistic impaction. Other X-Rays may be indicated. After accepting the patient and after the exam and X-Rays, treatment is initiated and that may include certain therapies to inhibit pain in addition to manipulation of the spine.
*See our X-RAY page for more information on “Essentials of Skeletal Radiology”, and Terry Yochum, DC, DACBR. ** If X-Rays were taken elsewhere, we will make every attempt to obtain those films, interpret them and render a professional report on said outside films. If the outside films or reports simply can’t be found for whatever reason, we usually proceed with our own set.

It must be noted that the acceleration-deceleration movements of the neck are typically completed within 250 milli-seconds. The astounding brevity of the time frame precludes any voluntary or reflexogenic muscle response that might arrest, limit or otherwise exert some control on the movements of the Cervical motion segment. This sets the scene for a variety of injuries. (Lord, “State of the Art Reviews, Cervical Flexion-Extension/Whiplash Injuries”, Spine & Hanley & Belfus, 9/1993. Teasell & McCain, “Painful Cervical Trauma”, Williams & Wilkins, 1992. Havsy, “Whiplash Injuries of the Cervical Spine and Their Clinical Sequelae”, Am J of Pain Management, 1/94. )
Timing:
Often is the case where a patient will feel a bit of pain at the time of the accident or no pain at all. Later, various pain issues will occur several hours, days, a week or even months AFTER the initial impact. Delayed reactions are the norm, not the exception in whiplash injuries according to the literature. In fact, there are no published reports I am aware of that say otherwise. (Foreman & Croft, ibid). There has been some research to show that after this, or any kind of serious trauma, the body’s natural opiate system kicks into gear. The pituitary gland and hypothalamus both initiate the release of “endorphins.” These are natural pain killing opiates that your own body generates and releases after trauma. The initial release of these endorphins would explain why people don’t seem to have pain until after several days. (Vernon HT, Dhami MS, Howley TP, Annett R, “Spinal manipulation and beta-endorphin-a controlled study of the effect of a spinal manip. on plasma beta-endorphin levels in normal males”, J Manip. Physio. Ther. 1995, 18 (8): 530-6). Delayed reactions to pain after car accidents IS widely cited. Here are a few: Farbman A, “Neck Sprain:Associated Factors”, JAMA, 1973, 223 (9): 1010-1015; Hirsch S, Hirsch P, Hiramoto H, et.al., “Whiplash Syndrome: Fact of Fiction?”, Ortho. Clinics of North America 1988, 19 (4); Gay, J, Abbott K, “Common Whiplash Injuries of the Neck”, JAMA 1953, 152 (18): 1698-1704;

Car Damage v. Human Body Damage:
Another popular myth concerns car body damage. Specifically, the anecdotal thinking is that if the car doesn’t “look” too bad, then there must not have been any human body damage. More than half of all Whiplash injuries occur in crashes where there is little to no car damage. It is now widely known that car bumpers are engineered NOT to deform but rather give and recover up to 5 mph. Ironically, it was the insurance lobby itself that paid off Congress to pass laws that compelled auto manufacturers to make “low impact proof” bumper systems - not to save people of course, but to reduce car repair bills. As we shall see, there is still energy transferred into the car. If the bumper doesn’t crumple as most don’t now days in low impact collisions, the people in the car absorb the energy. The fact is, there is more whiplash now than ever before precisely because of the way cars are engineered.
The reality is this: Newton’s Laws of Linear Momentum hold true to this day. Which is to say, energy is transferred during a car crash. Even if the car that got hit (yours for example) doesn’t “look” too bad, there was still a huge amount of energy transferred from the impact that went somewhere.
People are suffering whiplash syndromes at epidemic rates these days precisely because cars are built like steel cages. The cars are designed NOT to crumple in most cases. Much like billiard balls; there is no physical damage but one ball stops and the other goes flying across the billiard table. This is known as “Elastic Collision.” The energy or momentum of the crash transfers into the car and the passengers get whiplashed even more than they did when cars used to crumple up like empty milk cartons. *That is referred to as “Plastic Collision”-where the car or cars crumple up.
The fact is, there is no statistical correlation between vehicle damage and patient outcome. (Macnab, in The Spine, Saunders, 1982 pg. 648; Hirsh, Whiplash Syndrome, Orthopedic Clinics of North America, 10/88, p. 791) **NB: Just today, for example (3/27/06), there was an article in the Boston Herald about a tragic car crash yesterday. The two restrained (i.e.. with seat belts) parents were killed instantly while the unrestrained 4 year old hardly had a scratch. The car rolled over and was half crushed. Here, the parents died while a 4 year old being thrown around inside emerged in generally great condition. It serves as yet another every-day example of the folly of trying to predict the who, why and how of MVC injuries. See also Robbins MC, “Lack of Relationship Between Vehicle Damage and Occupant Injury”, Soc. of Auto. Engineers, 1997; 970494.
It is well known that a favorite area of testimony by accident reconstructionists (at the behest of insurance companies) is to assert that a lack of damage to the vehicle bumper suggests that the occupants could not have been injured. It has given rise to the ridiculous euphemism “No Crash, No Cash.” More recently, insurance companies have created a legal strategy based on MIST (Minor Impact Soft Tissue) segmentation strategy. The MIST protocol calls for accidents producing less than $1000 in damage are to be adjusted for minimal compensation. Legitimate experts now acknowledge that this testimony is a MYTH since, after 1973, car bumpers were generally designed to absorb impact forces - not protect vehicle occupants; There is no validity to the argument that a jury should see a bumper photo because it reflects the damage to the car or lack thereof. “Plaintiff‘s Lawyers Guide to Minor Impact Cervical & Lumbar Injury”, Litigation One, 2001.
Also consider the following references: MacNab, “The Spine”, Saunders, 1982. ~MacNab tells us; “The amount of damage sustained by the car bears little relationship to the force applied.” Ameis, “Cervical Whiplash: Considerations in the Rehabilitation of Cervical Myofascial Injury”, ” Canadian Family Phys., 9/86. ~“Each accident must be analysed in its own right. Auto Speed and damage are NOT RELIABLE indicators.” Emori, “Whiplash in Low Speed Vehicle Collisions”, SAE, 2/1990. ~“ . . .neck extension becomes almost 60 Degrees which is a potential danger limit of whiplash, at collision speed as low as 2.5 km/h.” It is also now known that examination of the undercarriage of the car will usually yield more ballistic damage such as the car frame or the frame rail. The car bumper is the LEAST reliable indicator of car damage in low impact rear end collisions (LOSRICs).
A recent article by the venerable Arthur Croft, DC substantially answers this entire question: Is there a correlation between car body damage and human body injury? The answer, it seems, is a resounding NO. His sizable metanalysis covered all known, reliable literature on the subject going back to 1970. See Croft A, Freeman M, “Correlating Crash Severity with Injury Risk, Injury Severity, and Long Term symptoms in Low Velocity Motor Vehicle Collisions”, Med Sci Monit, Vol. 11(10), 2005.
Head-Restraint Geometry:
This has to do with how close or far the head rest of the vehicle that you suffered your accident in, was located with relation to your head. More than two inches away from the head and the efficacy of head restraints drops off significantly. Go to www.iihs.org (Insurance Institute for Highway Safety) to find out the crashworthiness of your car and the efficiency of your head restraint as rated by the Insurance Institute for Highway Safety.


Car Damage Photography:
What often happens in MVCs is that Accident Reconstructionists and/or an adjuster for the insurance company itself will take pictures of the car after an accident. In the LOSRIC scenario, where there “appears” to be little damage to the car, these photographs are used to deny a claim altogether or limit payments to people who have been injured. As we alluded to in the previous paragraph, simple photos of the outside of a car after a LOSRIC should NEVER be admitted as evidence in car accident settlement situation. To properly document a LOSRIC car accident, photos of the undercarriage of the car are needed. It is the frame and the frame rails of automobiles that are consistently warped and damaged in impacts of all velocities.
The IIHS (Insurance Institute for Highway Safety) has admitted that a significant portion of whiplash injuries occur with minimal to no visible car body damage. (Croft, ibid). The Supreme Court of Delaware ruled in Rosetta v. Franz Maute, No. 307, 2000, 770 A. 2d, 36, that crash photographs were inadmissible unless the lawyer displaying them brought in an expert to testify as to their significance and meaning to the case. Please do a search on the “DAUBERT DECISION” regarding the above. That case went a long way in establishing what can and cannot be presented as evidence at trial. Exceptions to this of course would be a LOSRIC with extensive, visible car body damage. Again, in this paragraph we are emphasizing the low speed rear impact collision scenario that often reveals minimal to no car body damage when the exterior of the car is casually viewed.
Early Treatment:
The literature is clear on this; early active treatment is far more effective than “doing nothing” as some have suggested. (Waddell, G, “A New Clinical Model for the Treatment of Low Back Pain,” SPINE, Vol. 12 (7), 1987; Volvo Award Winning Article. “There is remarkably little scientific or clinical evidence to support the value of bed rest for low back pain or even sciatica.”) Even now, in 2007, there are some doctors parading as “insurance consultants” who strongly suggest the do-nothing “strategy” for whiplash/CAD injuries.
It has been my experience in over 23 years of treating CAD injury patients that early, active management greatly alleviates future pain and scar issues. In a highly interesting article (Mealy, K, Brennan H, Fenelon, GCC, “Early Mobilization of Acute Whiplash Injuries,” Brit. Med. Journal, Vol. 292:8 3/1986), the authors clearly showed that early active care including movement/cavitation of the spinal joints was more effective than cervical collars and bed rest.
See also:
Kellet, J, Acute Soft Tissue Injuries-A Review of the Literature, American
C. of Sports Med., Vol 18 (5), 3/86. *Hard to find article
on the efficacy of early intervention with rehab and modalities in
acutely injured patients.
Schofferman, J, Wasserman, S, Successful Treatment of
Low Back Pain and Neck Pain after a Motor Vehicle Accident DESPITE
Litigation, SPINE, Vol 19 (9), 1994. ~ The conclusion here is that LBP or Neck Pain resulting from a motor
vehicle accident showed a statistically significant improvement WITH
treatment despite ongoing litigation.
Khan, S, Cook, J, Gargan, M, Bannister, G, A Symptomatic
Classification of Whiplash Injury and the Implications for Treatment,
J Ortho Med., Vol 21(1) 1999. ~ The conclusion here is that Whiplash is very common and the
Chiropractic is the only PROVEN effective treatment in chronic cases.
Furthermore, conventional treatment(medical and/or rest) is
disappointing.
Mooney, V, Where is the Pain Coming From? SPINE, Vol 12 (8), 1987.
~ The upshot here was about how heavily impregnated the intervertebral
disc is with nociceptors. It is a far reaching paper discussing things
such as chemoreceptors, many and varied other causative agents of pain
but he concludes with, “Prolonged rest and passive physical therapy
modalities no longer have a place in the treatment of this chronic
problem.”
Seat Belts:
It is now widely documented in the literature, that with the introduction of mandatory seat belt laws, there indeed has been a reduction in deaths and serious injuries after motor vehicle crashes (MVCs), but, there has been a significant INCREASE in neck sprains.
That’s right, a seat belt actually makes the soft tissues of the neck and pain issues more painful after a MVC. It does this by anchoring the body in place and thus allowing the head free, or in many cases, wild unrestrained movement during a car crash. Also, even with a shoulder strap in place, the body can rotate “out” of the protection area with the free shoulder leading the way thus causing even more injury. {Navin F, Romilly D, “Investigation into Vehicle and Occupant Response Subjected to Low-Speed Rear Impacts,” SAE, 1989, 159-168; Hirsch S, Hirsch P, Hiramoto H, et.al., “Whiplash Syndrome: Fact of Fiction?” Ortho. Clinics of North America 1988, 19 (4): 791-795; Porter K, “Neck Sprains After Car Accident,” Brit. Med. Jour., 1989, 298 (973-974); Evans, R, “Some Observations on Whiplash Injuries,” Neurologic Clinics 1992, 10 (4): 975-997.
Pre-Accident Degeneration:
Patients often already have pre-existing issues. The literature tells us that this will compound an injury. Pre-existing degeneration aka: “degenerative joint disease/DJD” should NOT be confused with the new injury itself. Often is the case where an opinion will be rendered stating the patient already had some degree of degeneration so any new pain or discomfort experienced by a motor vehicle crash is really just the old injury. This is NOT true! (Turkek, Orthopedics Principle and their Applications, Lippincott, 1977, p. 740; Calilliet, Neck and Arm Pain, F.A. Davis Company, 1981, p./ 103. Webb, “Whiplash: Mechanisms and Patterns of Tissue Injury,” J Australian Chiro. Assoc., 6/84. Mairmaris, “Whiplash Injuries of the Neck: a Retrospective Study,” Brit. J of Accident Surgery, 1988. Watkinson, “Prognostic Factors in Soft Tissue Injuries of the Cervical Spine,” Brit. J of Accident Surgery, #4, 1991.)
Dr. A. Croft, seen below lecturing.
Symptoms and/or Injuries resulting from a MVC:
The health issues and problems that arise after a MVC, particularly from Whiplash, are legion. We’ll list the more common and prominent pain and injury scenarios here; be advised, some may surprise you.
1) Brain
Injury:
Yes, brain injury. Believe it or not, brain injury occurs relatively
commonly as a result of the physical movement of the brain inside the
skull after impact. It is roughly similar to being struck in the head
several times during a boxing match. Biochemical reactions also occur
for up to 96 hours AFTER the the initial trauma. This involves the
formation of free radicals and other toxic bio-chemical reactions that
occur at the cellular level. The resultant symptoms usually manifest as
confusion, difficulty in concentration, sleep disturbances,
irritability, forgetfulness, excess anger, decrease in libido, altered
moods, etc. In fact, some studies have shown a permanent loss of IQ.
2) Cranial
Nerve Injury:
These are the nerves that exit the brain directly. These nerves are a
combination of sensory, motor or both. They control such things as
smell, sight, taste, facial function, tongue movement, shoulder
movement, scalp and internal organ function. Blurred vision is a common
complaint after an accident. Uncontrollable tearing, smell dysfunction
as in either a lack of the ability to smell and/or the sensation of
smelling something that isn’t in the area, blushing, irregular heart
beat, upset stomach. These are a few of the functions that are mediated
by the cranial nerves and can be adversely affected by a Whiplash
accident.
3) Dizziness:
A very common complaint after a MVC. This most often results from
injury to the joints of the cervical spine. Chiropractic care is
especially beneficial in relieving this problem. This due to the fact
that the vast majority of balance information sent to the brain comes
from the neck. Restoring the neck to proper position via chiropractic
adjustments is what chiropractors excel at. More serious complications
may arise causing dizziness through injury to the brain stem or the
brain itself. However, commonly, it is the so-called mechanoreceptors
of the cervical spine that detect our place in time and space. This
information is relayed to the central vestibular and reticular systems
in the brain for integration and balance coordination. If the neck has
been traumatized, the messages going to the vestibular system from the
neck will be aberrant and thus lead to dizziness. (see Guyton A, Hall
J, “Textbook of
Medical Physiology,” 10th Ed., 2000, pg. 645, W. B
Saunders Co.)
4) Headaches:
After basic neck pain, headaches are the next biggest complaint
patients speak of after a Whiplash. Most are related to neck injury and
the subsequent muscle spasm that occurs in the neck that then affects
the skull. Chiropractic excels in treatment of headaches of all
varieties as a result of Whiplash.
5) Neck
Pain:
By far, the single most prevalent complaint in a MVC is that of neck
pain. Over 90% of the patients studies reported neck pain after a
Whiplash. This often leads to shoulder, arm and upper mid-back pain.
Again, this condition, barring the unusual, is remedied nicely via
chiropractic care.
6) Low
Back Pain:
Another common and yet surprisingly misunderstood issue after a MVC.
Various studies have shown that even in cases of primarily Whiplash,
the low back is often involved; up to 50% of the time. Seatbelts are
often involved in the mechanism of low back pain in a car accident.
Why? Because the belt anchors a person to the seat while the upper back
and particularly the neck often get “whipped” in the accident which
aggravates the low back.
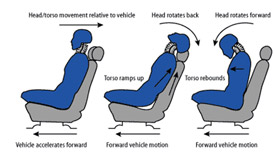
Additionally, there is the phenomena of “ramping” to consider. Ramping
is when the human body loads up on the seat back initially. In other
words, you, the passenger, tend to climb UP the seat back several
inches. The entire spine experiences a straightening of all curves and
as a result, there is compression of the spine. Ramping occurs in
almost all cars, yet the seat belt is anchored to the seat belt hooks
and thus, there is a tremendous amount of pressure put on the waist
line and low back as the seat belt attempts to hold the person down
while the force of the accident is pushing the person upward. Along
with this painful condition is the SI syndrome. This stands for
Sacro-Iliac joint. It is the hip joint that connects the upper body to
the hips and lower body. This joint is frequently pushed out of its
normal alignment. It is a gliding joint with a synovial lower section
and a fibrous upper section. Chiropractic manipulation is successful at
reducing this problem as well as low back pain.
7) TMJ:
This stands for Temporal-Mandibular-Joint. The mandible (lower jaw)
inserts itself into your skull via a notch in the temporal bone. This
hinge joint is your jaw joint, hence the name TMJ. This joint is
frequently injured in a MVC. Clicking and popping noises are often
found in the jaw joint after an accident. This condition is not as
common as the others mentioned but it is still seen frequently. This
condition is easily reduced with chiropractic care. As a matter of
fact, TMJ is often nicely reduced by manipulation to the neck WITHOUT
having to directly apply manipulative forces to the TMJ itself.
8) Blurry
Vision:
Still another normal concomitant of Whiplash/CAD accidents is blurry
vision. It is often the result of disrupted blood flow to the eyes
and/or aggravation to the “Sympathetic Nervous” system. This side
effect, thankfully, usually goes away within a day or two but it is
very disconcerting to the average accident victim.
Prognosis:
Over the past four decades, numerous studies have been undertaken trying to demonstrate and predict long term prognosis for Cervical Acceleration/Deceleration (CAD) injuries. Foreman & Croft analyzed this vast body of studies and excluded those lacking proper scientific methodology such as blinded studies, accurate descriptions of injury mechanisms and so forth. What remained are 43 scientifically reliable studies published in graph form in Foreman & Croft’s book, 3rd Ed. on page 408.
The literature is clear and consistent; virtually all existing research points to the same conclusion: long term affects can and do appear in CAD. People were shown to be suffering long term affects of CAD for months to YEARS after the fact. This body of literature based evidence cannot be ignored. In the alternative, there is NOT ONE study available that shows patients automatically heal within a few weeks after a CAD experience. Nor is there a single study that shows that people automatically heal after a CAD experience “with or without” treatment as is sometimes alleged by the “insurance consultants” and IE doctors. See also Davis C, “Chronic pain/dysfunction in Whiplash-associated Disorders,” J Manipulative Physio. Therapy (JMPT) Vol. 24 (1) 1/2001: p 44-51.
Another way of putting this is to consider the lingering effects of whiplash. In a great article gaining more and more coverage lately, the authors (listed below) brought to attention the following data:
- At a mean of 15.5 years post whiplash trauma, 70% of the whiplash injured patients continued to complain of symptoms referable and related to the original accident.
- Long term symptoms from whiplash injury include neck pain, arm paraesthesia, back pain, headache, dizziness and tinnitus (ringing in the ears).
- Women and older patients have a WORSE outcome from whiplash injuries.
- Between 10 and 15 years after the accident, 18% of the patient had improved, whereas 28% had deteriorated.
- Radiating arm pain is more common in those with severe symptoms.
- Soft-tissue injuries to the cervical spine may give persisting symptoms.
- Most whiplash injured patient reach their final state by two years after being injured, but this study showed ongoing symptom fluctuation between 10 and 15 years.
- At the 15 year follow up, neck pain was present in 65% and low back pain was present in 48% of the subjects investigated.
- 80% of women and 50% of men continued to have symptoms at 15 years.
- Back pain and tinnitus (ringing in the ears) actually INCREASED between years 10-15.
- Degenerative changes are associated with a worse prognosis for recovery.
- 60% of symptomatic patient had not seen a doctor (MD/DC) in the previous five years because the doctors were unable to help.
- Whiplash symptoms DO NOT improve after settlement of litigation.
- Chronic whiplash symptoms will cause an abnormal psychological assessment after 3 months.
- In this study, 100% of the patient with severe ongoing problems had cervical spine degeneration. *(Squires, B, Gargan, MF, Bannister, GC, “Soft-tissue Injuries of the Cervical Spine: a 15 year Follow-up,” J of Bone and Joint Surg. (British), Vol. 78B(6), 11/96, p 955-7. From the University of Bristol, England) **See also this companion study: Gargan, MR, Bannister, GC, “The Comparative Effects of Whiplash Injuries, ” J of Ortho. Medicine, 19 (1), 1997.
One additional article should be mentioned here as
well with regard to prognosis:
Berglund, A, Alfredsson, L, Cassidy, JD, et.al., “The Association Between
Exposure to a Rear-End Collision and Future Neck or Shoulder Pain: A
Cohort Study,” J Clin. Epid., Vol. 53 (11), 11/2000. ~Their conclusions were:
- i) 39.6% of those injured in a rear-end MVC have chronic neck pain 7 years later
- ii) A carefully matched control group who had never been injured in a MVC had neck pain prevalence of 14%
- iii) This 14% incidence of neck pain is probably equivalent to the incidence of neck pain in the general population
- iv) This means that there is an approximate 3X increased probability for neck pain for those injured in a MVC 7 years later
- v) Whiplash injury results in chronic neck pain in a large percent (40%) of those injured, 7 years after the injury
- vi) This chronic neck pain is organic, it is not related to malingering or compensation neurosis
- vii) The 2 Lithuania studies were flawed and the conclusions were erroneous.
Treatment:
For the majority of Whiplash/MVC cases, substantial relief can be found with chiropractic adjustments, supportive procedures like electrical muscle stimulation/ gentle traction/ early but limited use of pain inhibiting medications/procedures like ice and a cervical-orthopedic pillow. We quite like and often recommend the use of a specific orthopedic pillow for neck support while sleeping. It is low tech but highly effective for supporting the cervical spine and helping to restore/maintain the basic cervical lordosis.
As for pain medications, we usually suggests that the patient move off of them early in the course of treatment. This is because if a patient is too dependent on pain meds and gets too anesthetized by the medication, they will tend to continue their normal lifestyle routines which often actually cause more long term damage to the soft tissues of the body. By being aware of the pain and constitutional symptoms of a ballistic impact injury, patients can better modify their lifestyle to DECREASE stress to the tissues of their body.
Rehab is often used in this clinic to complete the therapy for the more severe cases of injury after a car accident. A more severe case of whiplash is indicated by persistent pain that lasts for a month and half or more as well as the physiologic status of being “De-Conditioned.” This suggests that the whiplash more extensively damaged the soft tissues, failed to lay down scarring along normal stress line and/or irritated local nerves.
Whiplash and similar injuries to the rest of the spine can also lead to discs rupturing in the neck like a “slipped” or herniated disc in the back. ’Chiropractic is a proven effective treatment in chronic whiplash cases’-Woodward MN, Cook JC, Gargan MF, Bannister GC, “Chiropractic treatment of chronic Whiplash injuries,” J. of Injury, 1996, 27 (9): 643-5; ’Another study of chiropractic treatment of whiplash injuries showed 75% of the patients improved following treatment,’ Khan S, Cook J, Gargan M, Bannister G, “A Symptomatic classification of whiplash injury and the implications for treatment,” J. Orthopedic Med. 1999, 21: 21-5.

Other symptoms from a car accident and whiplash may include radiating pain into the shoulder, elbow, wrist or hand. Likewise, there are many other factors in car crashes that could be discussed but would totally exceed the length of this one web page, such as whether or not the victim was male or female (females are more likely to be hurt worse), seat back stiffness, head rest placement, position of the head (was the victim turned sideways at impact), brake use or not, size of the car(s), impact vectors such as whether or not the victim’s car was hit head on/from behind, in the side, or on an angle, awareness of the impending accident or not and air bag deployment.
An article published in the Journal of Orthopedic Medicine in 1999 pointed out the superiority of chiropractic care for patients suffering from long term whiplash. The authors of the article noted that a previous study had shown that 26 of 28 patients, or 93 percent, of patients with chronic whiplash benefited from chiropractic care. In the authors’ own study, they interviewed 100 consecutive chiropractic referrals of patients with chronic whiplash. Their results also showed that of the 93 patients who remained in the study, 69 of them, or 74 percent, found improvement. The researchers concluded their opening comments with the statement, The results from this study provide further evidence that chiropractic is an effective treatment for chronic whiplash symptoms.
The standard textbook on this subject was written by two chiropractors. The book is considered the “Gold Standard” in analysis, diagnosis, research and treatment algorithms regarding whiplash. The name of the book, as already heavily referenced, is Whiplash Injuries: The Cervical Acceleration/Deceleration Syndrome by Foreman and Croft. A link to their web site: Spine Research Institute of San Diego.